
Report and accompanying case studies co-produced by Aberdeenshire Community Planning Partnership (CPP) and What Works Scotland, which offer descriptions and discussion of areas of emerging policy and practice as the CPP explores ‘putting Christie into action’ and opportunities arising from the Community Empowerment Act.
Download the report
Summary
This report and accompanying case studies offer descriptions and discussion of areas of emerging policy and practice as the Aberdeenshire Community Planning Partnership (CPP) explores ‘putting Christie into action’ and opportunities arising from the Community Empowerment (Scotland) Act 2015.
The report aims to help others involved in public services and policymaking understand more about what is happening, and why, in relation to this developing area of public service theory and practice.
1. Inquiring into ‘prevention’
The report follows several collaborative learning and action processes between CPP partners and What Works Scotland which illustrate the CPP’s ongoing work to develop multi-layered preventative partnership working and to consider what is being learned from this.
2. The developing context for policy and practice
The Christie Commission 2011 provides the rationale for this focus on the developing context for policy and practice. The Christie Commission argues for the need to prevent inequalities (wider social problems) to both create a fairer, more equitable society and reduce demand on public services in a time of constrained public spending. Partnership and participation are the key tools for achieving this.

Barriers to, and opportunities for, culture change. Click on the image to see a larger version
Early strategic thinking by Aberdeenshire CPP (October 2015) and a first Collaborative Learning Day (December 2015) organised by the CPP and What Works Scotland highlighted the challenges faced in developing relevant partnership, participation and prevention.
They pointed to the current challenge for the CPP of learning the ‘how’ of preventative partnership working. For instance, how to manage change, re-design services and support participation that can actually impact on local inequalities and other social problems. In effect, learning how to engage together on ‘wicked’ (complex) social problems.
3. Developing a clear focus on preventative partnership working
A second Collaborative Learning Day was organised by Aberdeenshire CPP, NHS Health Scotland and What Works Scotland (May 2016) to build on the emerging questions and challenges from the first.
The presentations provided the following material for later discussions on the day across the following topics:
- The evidence base: reducing health inequalities, improving population health, preventative spend:
- Points to upstream, system-wide approaches, e.g. fiscal, regulatory, legislative and whole population health (public health) as likely most effective in reducing health inequalities.
- Potential savings are most likely achieved in the longer-term rather than the shorter-term
- Preventative spend: shifting to preventative spend is challenging. Options include:
- Disinvestment – moving spending from existing (reactive) services to preventative approaches, e.g. through pooling budgets to generate more effective coordination.
- Public accounting procedures – changing the focus from the current financial year to longer-term, e.g. use of predictive analytics and rewarding services that take a longer-term view.
- External investments – alternative sources of finance (public, social, private) that can support transitions and ‘double-running’ of preventative approaches and reactive services.

Three emerging areas of challenge
- The CPP’s focus: on upstream, ‘whole population’ public health strategies and its Local Outcome Improvement Plan (LOIP) provides the opportunities for building preventative partnership working.
Three emerging areas of challenge arising from discussions at the Learning Day then provided the focus for further inquiry on the development of this form of partnership working:
- How to support effective, multi-layered partnership working?
- How to deepen understanding of the realities of ‘prevention’ and preventing inequalities?
- How to generate committed, creative approaches?
4. Learning from policy and practice case studies about preventative partnership working
Two case studies provide material for discussing the development of such partnerships.
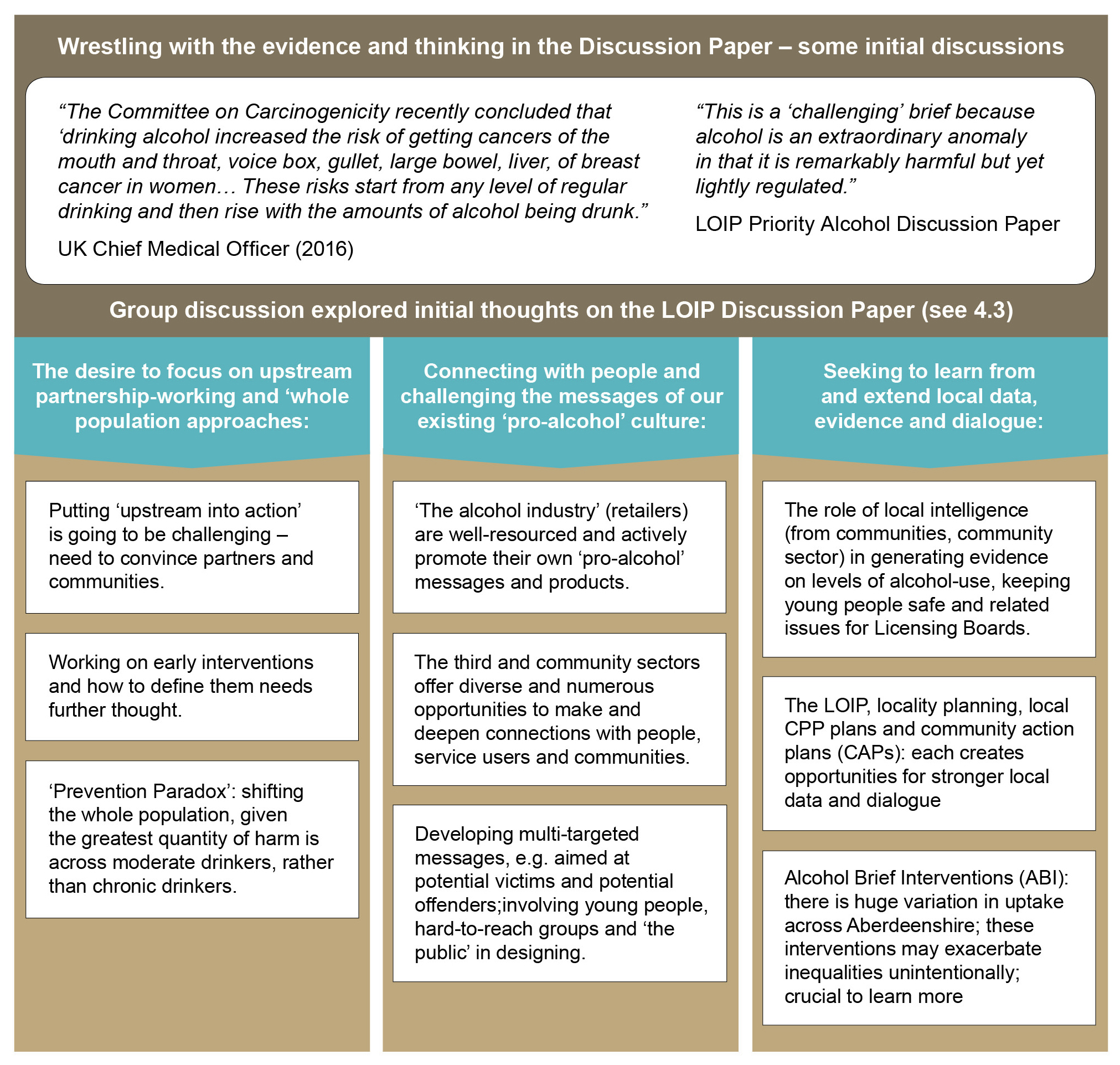
Case Study 1: A Changing Relationship with Alcohol
This case study describes early development work on a LOIP priority: changing Aberdeenshire’s relationship with alcohol. This was led by Aberdeenshire Alcohol and Drugs Partnership working with its CPP partners.
These graphics illustrate the wide range of issues, concerns and ideas that were generated for supporting the development of multi-layered preventative partnership working. (Click on the images to see larger versions).
-

- Mapping current partnership working

-

- Opportunities, issues & challenges raised

-

- Initial deliberations
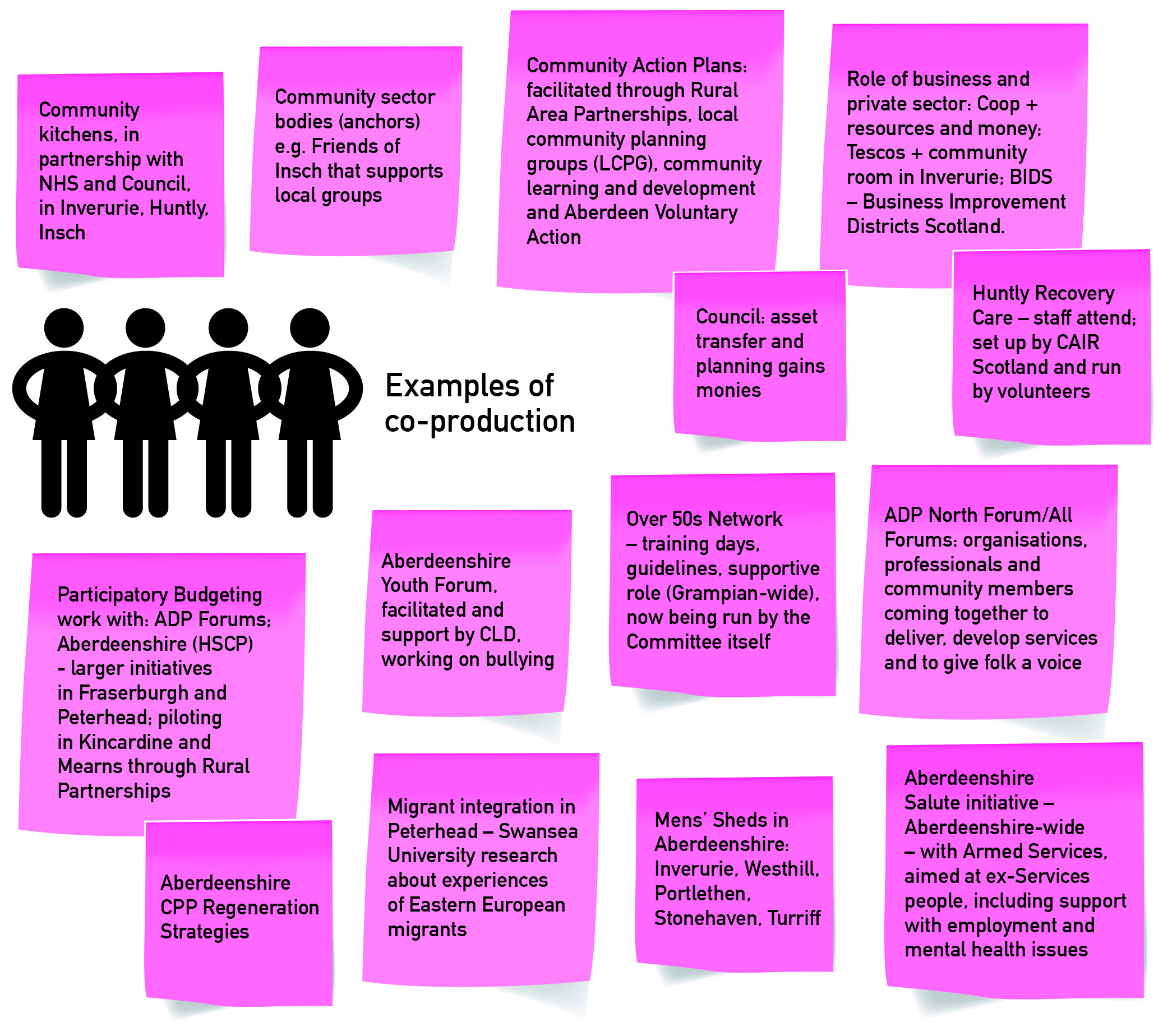
Case Study 2: Community Capacity-building for Health and Wellbeing
This describes on-going development work on a strategic approach to community capacity-building for health and wellbeing led by Aberdeenshire HSCP and working with its CPP partners.
These images show the initial mapping of community approaches and community capacity-building. (Click on the images to see larger versions).
-

- Examples of community organising

-

- Examples of voluntary action

-

- Examples of community enterprise

-

- Examples of co-production.
Emerging learning
The What Works Scotland commentary highlights the emerging learning from this early work:
Safe spaces for dialogue and deliberation are crucial
Both case studies illustrate how facilitated collaborative learning and action processes can provide a ‘safe’ context for shared dialogue on preventative partnership that builds understanding across diverse partners. There is potential to extend this into sustained externally-facilitated deliberation that supports an increasingly diverse range of public service and community partners in: considering evidence; exchanging reasons, emotions and values; and making informed, shared actions and plans (see, for instance Public Dialogue and Deliberation: A Communication Perspective for Public Engagement Practitioners, Oliver Escobar, 2011).
Deepening knowledge of ‘what works’
Working towards upstream, whole population and system-wide changes most likely to prevent inequalities (see Best preventative investments for Scotland – what the evidence and experts say – PDF, Neil Craig, 2014) is challenging for CPPs, particularly given their local focus on social problems often sustained by wider social and economic forces. Further, given the differing objectives of individual partner organisations there is the need to invest significant time in building relationships and shared understandings to support complex working. Access to suitable expert knowledge to support CPP partners in understanding the complexities of the evidence on prevention, partnerships and preventative spend would be invaluable.
Investing in preventative spend
Exploring opportunities to shift toward preventative spend was visible in smaller ways in the case studies as a focus on the role of community sector organisations that can coordinate local activity. This is a ‘new’ area of policy and practice and the opportunities outlined above (see 3. Developing a clear focus on preventative partnership working) suggest how policy and practice could develop to support preventative spend but these are not specifically illustrated in these case studies. The focus on the community sector within these two examples could, however, be developed further to support community enterprise and ownership that can generate (trading) income to invest in local economic and social development. The local community anchor organisation model offers one such route for this; the community-wealth model, with its mix of larger public bodies and smaller cooperatives, another.
Local democracy building
This is now a sustained national policy focus e.g. the Christie Commission, the Local Governance Review, the proposed Local Democracy Bill. Both case studies seek to explore the roles of community organisations, not only to generate local activity, but to support local dialogue, learning and build informed local commitment that engages with change. Such capacity could be harnessed to build local understanding and activity seeking to preventing inequalities.
Further reflections
Further reflections from policymakers and practitioners in this report consider:
- the importance of support for local decision-makers in using evidence
- the potential of local work (LOIP) on child poverty
- the need to build significant community infrastructure in low-income communities
Download the publications
- Executive Summary – Inquiring Into Multi-layered Preventative Partnership Working (PDF)
- Inquiring Into Multi-layered Preventative Partnership Working (PDF)
Get the case studies from the full report as separate publications:
- Multi-layered, Preventative Partnership Case Study: A Changing Relationship with Alcohol (PDF)
- Multi-layered, Preventative Partnership Case Study: Community Capacity-Building for Health and Wellbeing (PDF)
More details
Authors: Aberdeenshire Community Planning Partnership (CPP) partners and What Works Scotland
Type of publication: Collaborative research report
Publication date: March 2018
Related resources
Mapping the frontiers of collaborative governance
In this blog post James Henderson and Nick Bland from What Works Scotland discuss public service reform and how multi-layered preventative partnerships might address inequalities, drawing on the inquiry work for the report Inquiring into Multi-layered, Preventative Partnership.
Changing Aberdeenshire’s relationship with alcohol is a Local Outcomes Improvement Plan (LOIP) priority for Aberdeenshire Community Planning Partnership. In this blog post, Wayne Gault, Lead Officer with the Aberdeenshire Alcohol and Drug Partnership, reflects on how the Partnership approached the priority, what they have learnt from the experience, and what it means for practice.

Discover more about the collaborative inquiry work in Aberdeenshire, which has focused on two broad themes: community capacity-building for health and wellbeing; and using evidence across local and central community planning.